Deep
brain stimulation (DBS)
"Pacemaker of the Brain"
Obsessive-Compulsive Disorder (OCD) and Tourette's
syndrome Brain Treatments
|
|
|
Summary:
In 2009, Deep brain stimulation (DBS) was approved by the FDA to treat Obsessive-compulsive disorder (OCD). This FDA approval could be summarized this way, "We have no idea if DBS works, but since it doesn't kill people, you can experiment on live guinea pigs who are otherwise unresponsive to any other treatment for OCD. FDA approval opened the door for a large scale "clinical trial" of an unproven treatment. DBS is a form of ECT that shocks the brain with 5-10.5 volts through two 6 inch steel probes, that look like meat thermometers, which are pressed deep into the center of the brain. Although it is called a "Pacemaker of the Brain", such a comparison with an organ like the heart is absurd. A pacemaker keeps the heart beating in timing to the frequency of shocks applied to the heart. The heart naturally responds to such shocks of electricity. The brain, is more like a network cable between the body and the spirit. Applying random shocks of electricity to the brain is destructive and interferes with normal brain function. The brain runs on a natural voltage of about 1/10th of a volt. DBS shocks the brain with up to 10.5 volts, which is 100x the normal voltage the brain uses. Experts admit that the procedure is both experimental and unproven: "The effectiveness of this device (DBS) for this use (ODC) has not been demonstrated." (Neurostimulators for Psychiatric Disorders, Get the Facts, Medtronic inc.) "The long-term safety and effectiveness of brain stimulation therapy for obsessive compulsive disorder has not been established." (DBS Therapy For OCD, Implant manual, Lead Kit For Deep Brain Stimulation, Medtronic inc., 2009 AD, p 13) Since chemical psychiatrists are atheists who belief in evolution, they view man as nothing more than a pile of chemicals and electrons. They openly mock Christians who view the nature of man is dichotomous, having a distinct body and soul. This error has "dead ended" psychiatric research into insanity. They have wrongly look to the physical brain as the etiological cause of insanity for 300 years. Insanity happens in the spirit, not the body. A tiny clinical trial of 26 patients with ODC, demonstrated that the DBS implant actually increased OCD symptoms in 46.2% of the 26 patients. Any reported improvements could easily be accounted for through placebo effect. In 25 years, DBS will be put on the shelf beside all the other failed psychiatric treatments for insanity. (More: Deep brain stimulation)
Introduction:
- Deep Brain Stimulation was approved by the FDA for Essential tremor in 1997, Parkinson's disease in 2002, Dystonia in 2003 and for Obsessive-compulsive disorder (OCD) in 2009. Parkinson's and Dystonia are involuntary neurological malfunctions of the electrical system of the brain that can be seen in scientific tests and scanning. Obsessive-compulsive disorder is a voluntary disorder of free will and the human spirit and not a bodily disease of any kind.
- The brain is an electric organ and when you apply raw electricity to the brain, it is going to either damage or interfere with normal function of the body.
- "But the more lucrative application for DBS is as a treatment for refractory depression rather than OCD. As of late 2006, a number of groups are chasing success in this area. Unlike OCD, however, there is no consensus on what brain circuitry is affected in depression, and without such accord, many question whether the hazards of this treatment are worth pursuing for a condition that can often clear up miraculously without treatment. DBS may well offer benefits, but efforts to develop it, at least for depression, have the potential to inflict the kind of damage on psychiatry's current stock of physical therapies that psychosurgery inflicted in the 1950s, bringing the whole field to a standstill once more." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 283)
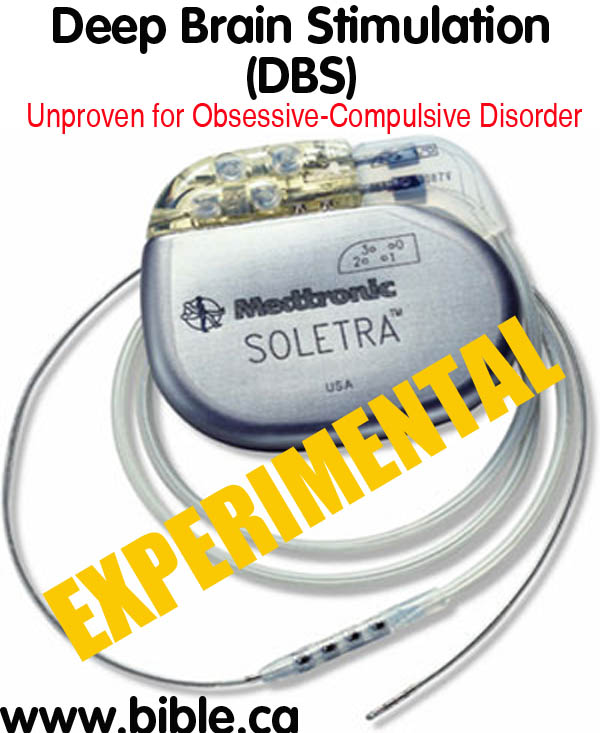
- Electrically shocking the brain has a long history in psychiatry and it has never worked. DBS is merely a milder, gentler way of shocking the brain: "Medtronic Reclaim DBS Therapy for Obsessive-Compulsive Disorder is approved under a Humanitarian Device Exemption (HDE) for people with chronic, severe, treatment-resistant obsessive-compulsive disorder. This therapy uses a surgically implanted medical device, similar to a cardiac pacemaker, to deliver electrical stimulation to precisely targeted areas of the brain. Electrical stimulation may help to reduce some of the symptoms of OCD. For Obsessive-Compulsive Disorder. Not everyone with OCD responds well to medication or cognitive-behavioral therapy. Reclaim DBS Therapy for OCD may relieve some of the symptoms of chronic, severe, treatment-resistant OCD. Neurostimulators are typically implanted near the collarbone. They generate electrical pulses and deliver them through extensions and leads to targeted areas of the brain. One or two Kinetra Neurostimulators or two Soletra Neurostimulators are used for Reclaim DBS Therapy for OCD. (Neurostimulators for Psychiatric Disorders, Get the Facts, Medtronic inc.)
- DBS is for those who fail to respond to any other kind of psychiatric treatment: "The Medtronic Reclaim DBS Therapy is indicated for bilateral stimulation of the anterior limb of the internal capsule, AIC, as an adjunct to medications and as an alternative to anterior capsulotomy for treatment of chronic, severe, treatment-resistant obsessive compulsive disorder (OCD) in adult patients who have failed at least three selective serotonin reuptake inhibitors (SSRIs)." (DBS Therapy For OCD, Implant manual, Lead Kit For Deep Brain Stimulation, Medtronic inc., 2009 AD, p 9)
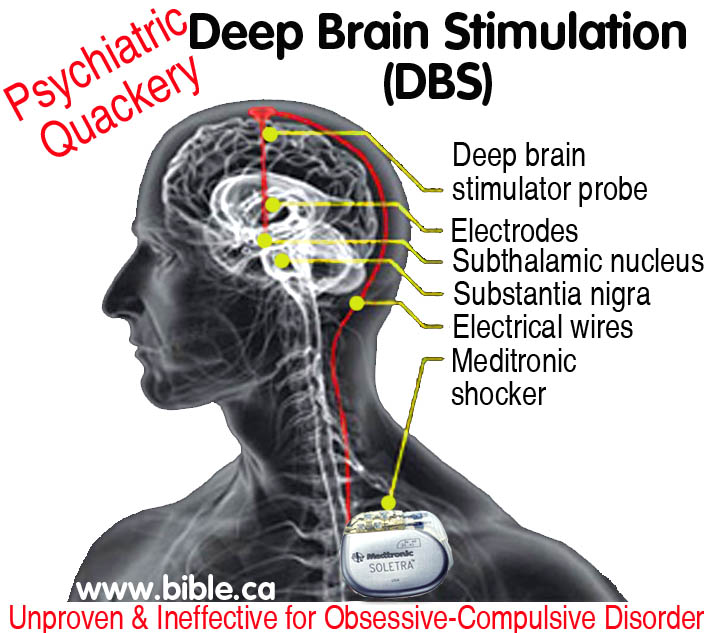
- Deep Brain Stimulation is unproven and ineffective for
Obsessive-Compulsive Disorder which requires two
steel rods, similar to meat thermometers, to be pushed deep inside
the brain to supply shock to both sides of the brain. "The Soletra
neurostimulator works with one extension and one lead. Two Soletra
neurostimulators are required for bilateral therapy, or stimulation of
both sides of the brain. Bilateral neurostimulation using two Soletra neurostimulators is approved for the
treatment of OCD." (Neurostimulators for Psychiatric
Disorders, Get the Facts, Medtronic inc.)

- "It appears that neither psychiatrists, nor the editors of medical and scientific publications, nor the media, nor the public feel the need to reconcile the contradiction of treating the same brain disease with interventions as different as ECT, VNS, DBS, TMS, antidepressant drugs, cognitive therapy, various "talk therapies," and dolphin therapy. At this point, it may be well to recall that the so-called effectiveness of this kind of therapeutic hocus-pocus had been investigated more than two hundred years ago by some of the greatest scientific figures of the time who had no difficulty concluding that the miracle-cure they were examining—Mesmerism—was simply bogus. Just as importantly, they also concluded that because healer and healed are equally deceived and self-deceived, the effectiveness of the hocus-pocus therapy appears real, at least for a while. Then, after they are debunked, they lose their effectiveness and are soon replaced by new miracle cures. Mesmer first used magnets to cure patients. Then his mere touch turned out to be curative. Finally, he didn't even have to touch patients to cure them—they could cure themselves and each other by means of rituals that utilized the powers of an imaginary magnetic fluid, a property of "animal magnetism." Between 1774 and 1777, in a mere three years, Mesmer rose from obscure physician to world-famous healer, only to be exposed as a quack." (Coercion as Cure, Thomas Szasz, 2007 AD, p 148)
- While DBS may provide some positive correction for the electrical malfunctions of the brain and the associated involuntary motor muscle movement in diseases like Parkinson's or epilepsy, it has no value in voluntary motor movements that are called Obsessive-compulsive disorder. The motor movements associated with OCD have their origin in the human spirit and are conscious choices a person makes. The spirit sends signals to the brain to make an eye blink or repeat an action. Shocking the brain for OCD is no more effective than shocking the USB cable connecting a computer to the printer. The brain is merely the connecting cable between the human spirit and the physical body.
A. DBS for OCD is ineffective & doesn't work for depression:
- "The effectiveness of this device for this use has not been demonstrated." (Neurostimulators for Psychiatric Disorders, Get the Facts, Medtronic inc.)
- "VNS is far from being the only problematic new treatment on the block, however. The late 1990s also saw the emergence of deep brain stimulation (DBS), a treatment linked to what may be potentially even greater problems than those related to VNS." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 280)
- A small study of 26 patients was used to evaluate the effectiveness of DBS with OCD. Any reported improvements could easily be accounted for through placebo effect. DBS is a rather extreme form of treatment and patients know they are test guinea pigs of a new and experimental treatment. Therefore both patients and doctors, are more likely to report positive benefits of DBS. Since OCD is something entirely within the realm of freewill and personal choice of action, the placebo effect of DBS can be a powerful and predicable motivation for people to stop OCD behaviors, in spite of their normal brain function being hindered by random electric shocks through DBS.
- "Long-Term Safety and Effectiveness - The long-term safety and effectiveness of brain stimulation therapy for obsessive compulsive disorder has not been established." (DBS Therapy For OCD, Implant manual, Lead Kit For Deep Brain Stimulation, Medtronic inc., 2009 AD, p 13)
- "Warnings: Electroconvulsive Therapy (ECT) - The safety of ECT in patients who have an implanted deep brain stimulation (DBS) system has not been established. Induced electrical currents may interfere with the intended stimulation or damage the neurostimulation system components resulting in loss of therapeutic effect, clinically significant undesirable stimulation effects, additional surgery for system explanation and replacement, or neurological injury." (DBS Therapy For OCD, Implant manual, Lead Kit For Deep Brain Stimulation, Medtronic inc., 2009 AD, p 11)
- All psychiatric treatments for insanity, mental illness or
obsessive compulsive disorder (ODC), that shock the brain with electricity
as a cure, are utterly worthless, apart from the placebo effect, because
insanity is a spiritual problem, not a physical disease. Applying
electricity to the brain to cure insanity, is like applying household
electricity to your computer's central processor to fix a software issue.
Using ECT, rTMS, VNS, DBS is about as effective as fixing your computer
with your car jump starter! The human brain is the hardware, the software
is located in the spirit.

- Of course this doesn't surprise Christians, who understand that man has a spirit that is distinct from his body. The Christian understands from the Bible story of Luke 16:21, that when we die and our brain becomes dust, that we retain our memories, will, desires and emotions. Depression is a spiritual problem, not a physical disease.
- This device is absolutely unproven and is highly experimental. Since obsessive compulsive disorder (OCD) has its origin in the freewill choices of the human spirit and not the physical body, it should be rather obvious that shocking the brain is pure psychiatric quackery!
B. Side effects of DBS for OCD:
- First, you notice that the study is for a tiny total of 26 patients.
- Second, you notice that 100% of the 26 patients experienced some kind of bad side effect.
- Third, you notice that the DBS actually increased the OCD symptoms in 46% of the patients. That is a stunning failure.
|
Reported Adverse Events: |
||
|
|
Number of Events |
Number of 26 subjects affected (percentage of total) |
|
Therapy-Related totals |
188 |
23 (88.5%) |
|
Increased OCD symptoms |
22 |
12 (46.2%) |
|
Increased anxiety |
19 |
11 (42.3%) |
|
Insomnia |
18 |
12 (46.2%) |
|
Increased depression/ suicidality |
13 |
10 (38.5%) |
|
Cognitive disturbance (clouding) |
11 |
8 (30.8%) |
|
Induced muscle contraction |
10 |
7 (26.9%) |
|
Hypomania |
9 |
9 (34.6%) |
|
(DBS
Therapy For OCD, Implant manual, Lead Kit For Deep Brain Stimulation |
||
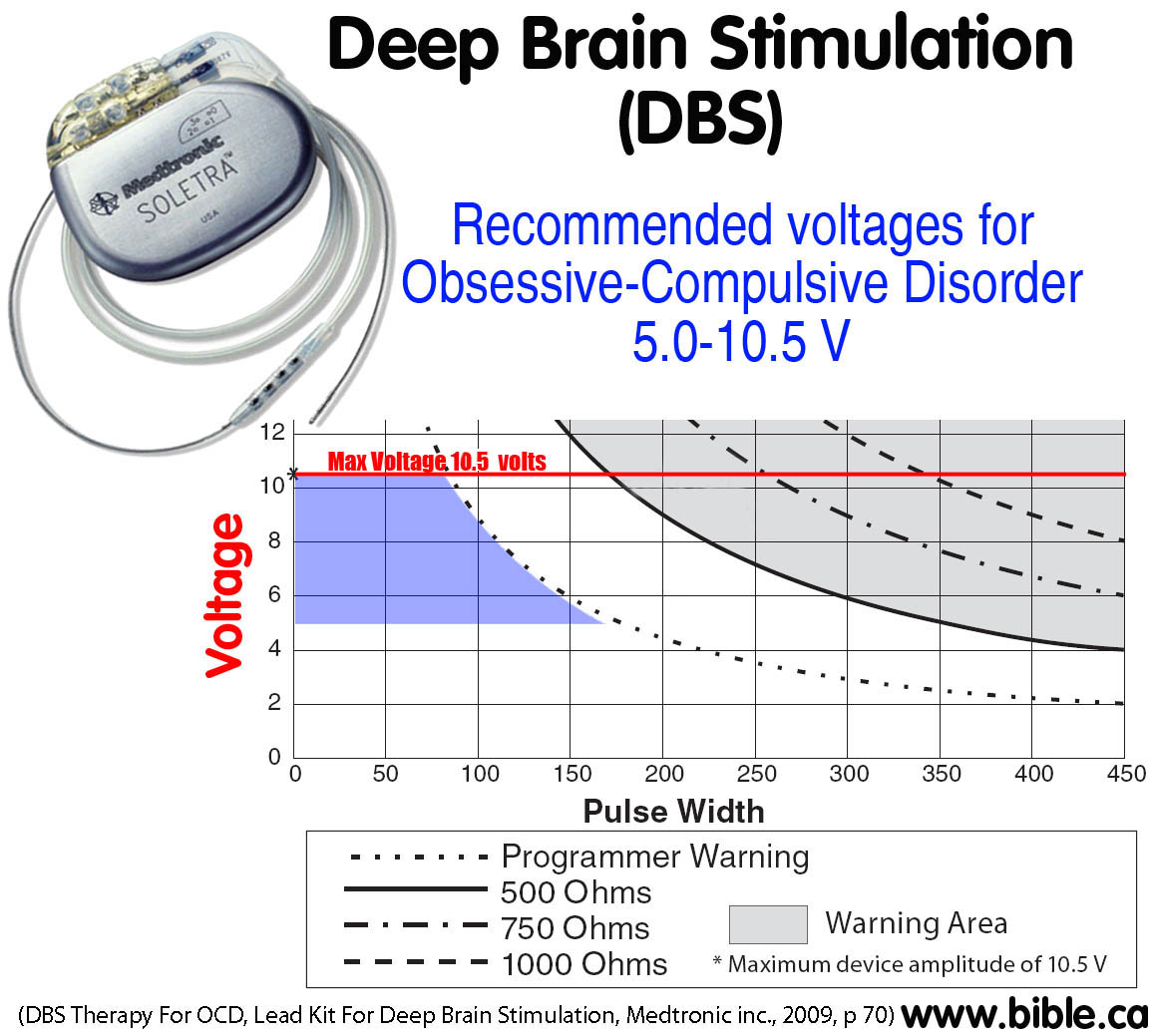
C. The shock of Deep Brain Stimulation: 10.5 volts
- All electric treatments in psychiatry use simple electricity... the same stuff your curling iron or a flashlight uses ... the same stuff your brain uses. It is simple electricity.
- The literature you read on DBS says that a tiny amount of electricity is used to shock your brains and nerves. However, the question is this: tiny compared to what? 10.5 volts is a tiny amount of electricity for a car, but would cause the CPU of a computer to internally explode! We are talking about your brain that runs on 1/10th of a single volt of electricity. Compared to the 450 volts that ECT shocks directly between the temples, 10.5 volts is a Sunday stroll in the park! But 10.5 still represents applying 100x higher voltage than the brain normally runs on natrually.
- "There is a potential risk of tissue damage using stimulation parameter settings of high amplitudes and wide pulse widths. ... The safety of somatic psychiatric therapies using equipment that generates electromagnetic interference (e.g., vagus nerve stimulation) has not been established." (Neurostimulators for Psychiatric Disorders, Get the Facts, Medtronic inc.)
- "Specifications for Soletra, Model 7426: Voltage: 0 to 10.5 Volts in increments of 0.1 V. Rate: 28 settings, 2-185 Hz (pps) - 5 values above 130 Hz. Pulse Width: 10 settings, 60-450 milliseconds." (Neurostimulators for Psychiatric Disorders, Get the Facts, Medtronic inc.)
- However, doctors are instructed by the manufacturer that the optimum final voltage is between 5-10.5 volts: "Kinetra Model 7428 and Soletra Model 7426 Neurostimulator: Typical Final Settings: Amplitude 5.0-10.5 V. Pulse Width 90-210 milliseconds. Rate 100-135 pps." (DBS Therapy For OCD, Implant manual, Lead Kit For Deep Brain Stimulation, Medtronic inc., 2009 AD, p 70)
- If you were to power the brain with a battery, it would use a 1/10 of volt battery supply. That is how much voltage typically powers the brain. 0.1v. VNS applies 100 times more voltage than the brain normally uses. To put this into perspective, remember the time you fried your 120 volt hair drying when you traveled abroad? That was twice the voltage and look what it did! Remember the smoke? Imagine if you applied 100 times the voltage to your hair drying (12,000 volts)! DBS shocks the human brain and nervous system with 100 times higher voltage than it normally operates on.
- You might wonder how much "shock" 10.5 volts feels like. Well fortunately, you can try it yourself by simply touching your wet tongue to a 9 volt battery. But first, touch the battery with your dry fingers. Then with wet fingers... then touch it to your tongue. A nine volt battery is 9 volts @ 2 ma when you touch it to your tongue. This is about the same voltage and current as the shock that DBS delivers to the human brain.
|
|
|
The Medtronic Soletra DBS brain shocker puts out about the same
electricity as what you feel when you touch your tongue to a 9 volt battery. 9v battery: 9 volts @2 ma |

D. Deep Brain Stimulation and Parkinson's Disease:
- Parkinson's disease (PD) is a physical electrical problem with the brain that has its etiological origin in the body, not the mind.
- PD is not a mental disorder or insanity, but a "dumbing down" of a person's awareness and ability to solve basic problems. "The most commonly reported neuropsychological finding in PD is impaired executive functioning. Executive functions include the ability to plan, initiate, and monitor behavior, as well as think abstractly, solve problems, and adapt to novel environmental stimuli. The myriad of difficulties in this domain is collectively referred to as dysexecutive syndrome and reflects underlying cortical and subcortical pathophysiology. Compared with groups of healthy controls, clinical samples of patients with PD demonstrate significantly more impaired performance on measures of executive functioning." (Deep brain stimulation for Parkinson's disease, Gordon Baltuch, Matthew Stern, 2007 AD, p 248)
- "When physical treatments like DBS were initially applied to Parkinson's disease, clear and relatively discrete brain circuits were sought as sites for stimulation. But this did not necessarily mean that those involved in the field were seeking to attack the root of the illness. Many researchers readily conceded that all they may be doing is to produce compensatory responses, or indeed inducing further brain dysfunction, in order to balance out the original disturbance, whatever that might be. For instance in Parkinson's disease, the stimulation of the subthalamic nucleus produces therapeutic effects but does not do so by correcting the initial abnormality. The effect is to produce a compensatory lesion that, as it were, rebalances the system rather than corrects the problem." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 287)
- DBS, is still considered an experimental treatment with no hard proof it works: "Given that STN DBS techniques for PD are in their relative infancy and equivocal results of observational studies, the true impact of STN DBS on cognition in patients with PD is unclear. ... The lack of data on such an important outcome variable is disturbing, given that the motor, psychiatric, and cognitive concomitants of PD may lead to social embarrassment, loneliness, and dependence on others for functionality. ... Although several reviews suggest that STN DBS does not have a deleterious effect on cognition in PD patients, and may actually improve functioning in some domains, there are insufficient data regarding the magnitude of the effects (positive or negative) of the procedure on cognition in patients with PD." (Deep brain stimulation for Parkinson's disease, Gordon Baltuch, Matthew Stern, 2007 AD, p 253)
- DBS is believed to work in cases of PD, by shorting out the electricity of the brain in areas where electrical malfunctions happen. It is called, creating a "lesion" or "overriding of pathological BG (basal ganglia) activity". "In summary, it seems most likely that STN (subthalamic nucleus) DBS works through a combination of mechanisms. It is generally believed that one of the primary mechanisms of DBS is the overriding of pathological BG activity, specifically bursting and low-frequency oscillations in the STN-GP network. The replacement of these activities with higher frequency regular spiking may represent an information lesion or may enhance "prokinetic" oscillations normally present in the healthy BG." (Deep brain stimulation for Parkinson's disease, Gordon Baltuch, Matthew Stern, 2007 AD, p 33)
- "DBS surgery is now an accepted and widely used procedure for management of patients with advanced PD complicated by motor fluctuations." (Deep brain stimulation for Parkinson's disease, Gordon Baltuch, Matthew Stern, 2007 AD, p 214)
- Since the involuntary shaking and bodily tremors are electrical disturbances caused by an electrical malfunction, DBS might theoretically be a way of lesioning (blanking out) and removing these symptoms. Some case studies make this theory promising: "Case Study 2: A 59-year-old women with a 13-year history of PD was operated on in late 2001 for a left DBS placement. Her symptom was a moderate right upper extremity tremor primarily on the right with some rigidity and bradykinesia, all of which became increasingly medication resistant. The surgical procedure was uneventful and IVIR1 targeting and microelectrode recordings (MER) assisted localization resulted in effective placement of the leads in the STN . Nine days after surgery her electrode was screened and programmed. Table 2 summarizes her programming sessions. The patient did not tolerate monopolar stimulation as she felt lightheaded. A "wide" bipolar setting was used and provided effective tremor relief. She was quite pleased with the result and did not return for programming for about a year when suddenly her left hand tremor reappeared. The Soletra stimulator was found to be off. Restarting the device controlled the tremor again and the patient was advised to regularly check the status of the device. Over time the patient' s left hand started to tremor to a point that made daily house work difficult. She was scheduled for a right DBS placement and several months later underwent a successful procedure. The new electrode was screened and programmed in monopolar mode during her hospital stay. The settings were increased in subsequent programming sessions. Two months later during the 6/12/02 visit, the patient complained about the persisting left upper extremity tremor. An increase in the monopolar setting from 1.7 to 2 V arrested the tremor but produced lightheadedness. So she was switched to bipolar mode at I —2+ then to 2-3+ as only approximately 90% tremor suppression was achieved on the former setting. At 4.5 V complete suppression was noted with no concurrent adverse events. On 3/19/2003. a small adjustment was needed to retain full tremor suppression. The patient was quite happy with the symptom control and did not return to the clinic until a year and a half later when suddenly her left hand was shaking worse than ever before. The battery for the left DBS device must have expired since no readings could be obtained with the n' Vision programmer (Medtronic 8840). She was scheduled as an outpatient for bilateral stimulator replacements, and following surgery both devices were reprogrammed before she left the hospital. An attempt was made to utilize more battery efficient parameters as seen in Table 2. Although full tremor control was achieved initially, several weeks later the settings had to he increased due to recurring tremors. Conclusions It is not always possible to limit the stimulation voltage to 3.6 V or less in order to optimize battery longevity. However, before voltages are increased beyond that threshold, it is advantageous to explore if a gradual increase in the frequency to 185 Hz, and possibly in the pulse width to 120 RS, would not yield additional symptomatic benefit." (Deep brain stimulation for Parkinson's disease, Gordon Baltuch, Matthew Stern, 2007 AD, p 125)
E. DBS disrupts normal brain function: "Lesions"
- When DBS shocks the middle of the brain, it disrupts normal brain function. This really is no surprise to any one who took the grade 9 introductory electricity course. In technical terms, this disruption is called a "lesion".
- Lesioning is like when your computer freezes for a moment during a power surge. All activity in the CPU stops while the power surge occurs. When the surge is over the CPU picks up where it left off.
- Electrical lesioning fixes a fibrillating heart. Arrhythmia is when the heart beats in an irregular or spasmodic rhythm. Atrial fibrillation occurs when the heart's electrical system makes the atria to quiver or "fibrillate". Different parts of the heart beat at different rates which means blood is no longer being pumped efficiently. The solution is a heart "Defibrillator" which we have all seen in emergency wards where the nurse puts two electrode paddles over the heart and on the side of the chest. "All clear", then zap! The shock makes the body jump off the bed, but the heart beat is reset back to normal rhythm. The is a prefect example of how electricity creates a lesion and saves a person's life. Applying "defibrillator" theory to correcting emotions by shocking the brain, is completely different matter and doesn't work.
- "As with TMS, DBS depends on neuro-imaging technology. In order to implant the electrodes in the correct location, it is necessary to be able to map each patient's brain in great detail using both MRI and CT scans, fusing these with computer programs to get a precise fix on the path of nerve tracts and blood vessels. A misplaced electrode can cause hemorrhage and death. The 2004 remake of The Manchurian Candidate gives a reasonably accurate image of what the procedure looks like. When the electrodes are in place, a battery operated device produces a stimulation that can be increased or decreased in frequency based on feedback from the patient. This stimulation can theoretically work by either overstimulating nerve cells, leading to somatic fatigue, or jamming the nerve cells so signals do not get through, in either case producing a functional lesion." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 281)
- "When physical treatments like DBS were initially applied to Parkinson's disease, clear and relatively discrete brain circuits were sought as sites for stimulation. But this did not necessarily mean that those involved in the field were seeking to attack the root of the illness. Many researchers readily conceded that all they may be doing is to produce compensatory responses, or indeed inducing further brain dysfunction, in order to balance out the original disturbance, whatever that might be. For instance in Parkinson's disease, the stimulation of the subthalamic nucleus produces therapeutic effects but does not do so by correcting the initial abnormality. The effect is to produce a compensatory lesion that, as it were, rebalances the system rather than corrects the problem." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 287)
F. DBS and Tourette's syndrome
- Tourette's syndrome is where a person experiences seemly involuntary motor ticks and various nervous habits like blinking, grunting etc.
- Several people with Tourette's have had the DBS imbedded in their brains.
- Some reduction in ticks was reported is some patients, but this is likely due to the placebo effect rather than the DBS device itself.
- Many patients reported no improvement and some rather negative side effects.
Conclusion:
- Obsessive-Compulsive Disorder (OCD) happens in the spirit, not the physical body.
- Deep brain Stimulation for OCD is pure junk pop-psychiatry
and makes the "junk psychiatry O-meter"
go crazy!
 (Left: Junk pop-psychiatry O-meter going crazy)
(Left: Junk pop-psychiatry O-meter going crazy) - The entire application of DBS to psychiatry is entirely theoretical and unproven.
- "Time will tell whether another chapter in the history of shock therapy is being written today or not. The history of the past sixty years has been a history of successive attempts to improve ECT. All have failed, even if individual lives were helped along the way. The treatment that Cerletti described in 1938, plus a few modifications involving muscle relaxation and wave form, is still with us today, and a row of bright ideas about magnets, nonconvulsive applications of electricity, and the like have not succeeded in making patient care better or safer. It remains to be seen if the current therapies will provide more convincing alternatives." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 289)
- DBS has some important applications in treating known physiological diseases like Parkinson's and epilepsy. The difference between epilepsy and depression is that you can conduct scientific tests to diagnose for epilepsy, but not for depression. Epilepsy is an electrical problem with the brain that causes involuntary motor control of the body. OCD is a spiritual choice made in the mind, that causes voluntary motor actions in the body.
- The error of chemical psychiatrists, is rooted in their atheistic belief in evolution that man is nothing more than a pile of chemicals and electrons. They openly mock Christians who view the nature of man is dichotomous, having a distinct body and soul. This error has "dead ended" psychiatric research into insanity in the physical brain as the etiological cause of insanity for 300 years. Insanity happens in the spirit, not the body. "It is not important whether this cerebroversion hypothesis is correct; the point is to highlight modern psychiatry's failure of imagination. At the start of the twenty-first century, thinking has been dominated by "bio-babble," a discourse characterized by jargon and an emphasis on the monoamines, dopamine, serotonin, and norepinephrine. Within a few years, this will almost certainly seem as vacuous as Freudian notions about libido. The problem, in the meantime, is that just as psychoanalysis once inhibited a generation from making progress in understanding what mental disorders are, so too psychopharmacology has held back development in theoretical aspects of psychiatry, at the expense of patients." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 296)
- Compared to ECT, DBS is the "new kid on the block" that is has captured researchers attention to find some treatment for Obsessive-Compulsive Disorder. They will fail when they look for the problem in the physical body.
- At present, there is no evidence DBS has any more effect on curing ODC, or any mental illness, than might be expected as the placebo effect.
By Steve Rudd: Contact the author for comments, input or corrections.
Send us your story about your experience with modern Psychiatry